
Scleroderma and Lupus
Scleroderma is one of the most common “overlap diseases” for those living with lupus, with about 20% of those with scleroderma also having lupus. Learn about the complexities of scleroderma including its symptoms, possible complications and the most common ways to manage this autoimmune disease.
- Introduction
- Types of Scleroderma
- Symptoms of Scleroderma
- Causes of Scleroderma
- Scleroderma as an Overlap of Lupus
- Diagnosing Scleroderma
- Treating Scleroderma
- In Conclusion

Introduction
Scleroderma is a connective tissue autoimmune disease that develops when parts of the body produce and accumulate too much collagen. Collagen is a fibrous protein that is responsible for providing structure and elasticity to certain connective tissues of the body, such as skin and cartilage. As an example, it is the loss of collagen that can cause an increase of wrinkles in the skin. However, when an individual has scleroderma, the skin of the hands, fingers and face may become thick and tough because of the over-production of collagen. Vascular involvement, such as vasculitis, can also occur and blood flow to the skin and organs may be restricted.
Relatively rare, scleroderma afflicts approximately 1 in every 1,000 individuals in the U.S., though many more individuals may have undiagnosed scleroderma. As with lupus, the incidence of scleroderma is higher in people of color. The disease typically affects individuals between the ages of 25 and 55 (slightly older than for lupus), and women are four-times more likely to have it than men. Children can develop scleroderma, though only about 2% will have symptoms before the age of 10.
About 20% of individuals with lupus will develop scleroderma; it is the most common of the lupus overlap diseases.
Types of Scleroderma
There are two types of scleroderma: localized and systemic.
Localized scleroderma affects the skin, but not the internal organs. As it spreads, fibrous tissue replaces what was once normal, healthy and supple skin. Skin lesions may also erupt, as skin tends to crack when it is affected.
There are three types of localized scleroderma:
- Generalized Morphea: This produces rough, dry, discolored patches of skin anywhere on the trunk, head, face and/or neck, and the patches tend to blend into each other;
- Circumscribed Morphea: This type produces rough, discolored, oval-shaped patches of thick skin on the arms, legs, trunk, head, face and/or neck; more severe morphea can appear all over the body (pansclerotic morphea); and
- Linear Scleroderma: This form is frequent in children under the age of ten and appears as thick bands or streaks of dry, thick and rough skin that may also develop as patches; this form of localized scleroderma can also affect a child’s bones and muscles, causing physical underdevelopment as the child grows.
Like lupus, scleroderma can become systemic (systemic sclerosis – SSc) by affecting internal organs as well skin. The lungs, heart, esophagus and kidneys are particularly vulnerable to SSc as they, too, can develop thick, fibrous scar-like tissue (fibrosis). Individuals diagnosed with scleroderma must be carefully monitored, as the condition can sometimes progress to SSc rapidly.
There are three types of systemic sclerosis:
- Limited SSc (also known as CREST syndrome): This appears on the head, face, fingers or possibly forearms; it rarely affects the organs, though some individuals may develop gastrointestinal issues and pulmonary hypertension;
- Diffuse SSc: This appears in patches on larger areas of the body and can affect the muscles and bones as well cause pain; the organs may become involved, and blood pressure may rise which can impact kidney function and cause damage; and
- Sine SSc: This type does not manifest on the skin, but can affect almost any internal organ and usually initially presents as Raynaud’s phenomenon.

Symptoms of Scleroderma
One of the most frequent and earliest signs of scleroderma is the presence of another lupus overlap disease, Raynaud’s phenomenon. Raynaud’s phenomenon affects the smaller blood vessels that supply blood flow to the skin causing them to constrict. As a result, parts of the body, such as fingers, toes, ears or even the nose can become cold, numb and even change color when exposed to cold temperatures and/or stress. Approximately 95% of individuals with scleroderma also have Raynaud’s phenomenon. According to a 2016 European Scleroderma Trials and Research Group (EUSTAR) study, other symptoms of scleroderma typically manifest in less than a year after the onset of Raynaud’s phenomenon.
Other signs and symptoms of scleroderma include:
- Skin manifestations: As mentioned earlier, the first sign of scleroderma is the appearance of fibrous skin on the hands, limbs and possibly face. Skin can appear tough, tight and shiny as it becomes thicker and restricts movement. Changes to skin coloration/pigmentation can occur. Red dots and/or lines may develop on the affect area, though not painful. Small bumps of calcium deposits (calcinosis) may also develop under the skin, and these can be painful. Unlike lupus, scleroderma does not produce sun sensitivity.
- Gastrointestinal upset: Individuals with scleroderma may experience heartburn and esophageal issues, which according to a 2016 EUSTAR study, is the most common gastrointestinal symptom. Intestinal issues may include diarrhea, cramping, bloating and constipation. It may also become difficult to absorb much-needed nutrients as a result of food being unable to properly digest along the gastrointestinal track.
- Pulmonary complications: Shortness of breath, the buildup of scar tissue on the lungs (pulmonary fibrosis), and pulmonary hypertension are the most common pulmonary symptoms of scleroderma. Lung disease, specifically pulmonary hypertension, is the leading cause of death in individuals with scleroderma. A 2018 Journal of Rheumatology study found that individuals who also have lupus have a higher incidence of experiencing pulmonary hypertension.
- Heart involvement: Diastolic dysfunction is the most prevalent cardiac symptom of scleroderma. Diastolic dysfunction occurs when the heart cannot relax in between beats so that the ventricles do not expand properly and fill with blood. This is due to the thickening and hardening of the muscles around the heart. This may also block the flow of electrical impulses through the heart (conduction blocks), and fluid may build up in the membranous sac around the heart (pericardial effusion).
- Renal problems: Though rare, kidney damage may occur as the blood vessels of the kidneys change. These changes can cause blood pressure to increase, which in turn can cause kidney damage. An individual may be completely unaware of the changes occuring in their kidneys, making it imperative for healthcare practitioners to carefully monitor individuals with scleroderma. Damage may occur within the first year or two of a scleroderma diagnosis.
Researchers of a 2019 study acknowledge that because SSc can be such a complex condition that can dramatically effect quality of life, registries need to be developed to track the diversity of disease expression and disease development. Tracking this information will help clinicians and researchers develop better diagnostic and treatment tools as well as more accurately measure outcomes and provide optimal care.
Causes of Scleroderma
As with many autoimmune and connective tissue diseases, it is unclear as to what specifically causes scleroderma. Researchers, however, have determined that the following may play a key role in who develops scleroderma:
- Genetics and Heredity: According to the Mayo Clinic, genetics and heredity may predispose an individual to develop scleroderma. Individuals with a specific gene profile may develop the disease – members of the same family often have the same unique profile. According to the U.S. National Library of Medicine, variations in two genes (IRF5 and STAT4), which are involved in immune function, may play a role in the development of scleroderma. It is also interesting to point out that the Mayo Clinic mentions that these gene variations are also more prevalent in certain ethnic groups such as the Choctaw Native Americans. These individuals are also more likely to develop SSc that involves internal organs.
Research shows that cytokines may trigger scleroderma symptoms. Cytokines are proteins involved in immune system responses in other autoimmune diseases such as lupus. Specifically, the pathways for type 1 interferons (1 IFN) seem to be activated in the presence of lupus and SSc, suggesting that they may be implicated in scleroderma.
- Environmental factors: Harvard Health suggests that tryptophan (an amino acid), when formerly used as a dietary supplement, could trigger scleroderma. Exposure to chemicals such as rapeseed oil, vinyl chloride and epoxy resins may also cause scleroderma symptoms. Men who were exposed to silica in coal mining have also developed the disease as a result of their exposure.
Researchers at the Poznan University of Medical Science in Poland summarized that several drugs may also induce scleroderma. Bleomycin, a drug used in chemotherapy, is reported to induce symptoms as well as paclitaxel (chemotherapy agent), pentazocine (analgesic), and appetite suppressants amphetamine, dexamphetamine and phenmetrazine.
- Other autoimmune diseases: Lupus, rheumatoid arthritis and Sjögren’s syndrome may also put an individual at risk of developing scleroderma.

Scleroderma as an Overlap of Lupus
As mentioned, if an individual already has an autoimmune disease such as lupus, they may find themselves facing other autoimmune diagnoses such as scleroderma. Researchers estimate that between 14% and 20% of individuals with lupus may also get scleroderma. These individuals typically present with Raynaud’s phenomenon more frequently as well as report having “discoid lupus, lupus nephritis, pancreatitis, avascular bone necrosis and shrinking lung syndrome.” Some researchers have determined that when an individual has lupus and is symptomatic, healthcare practitioners seem to diagnose scleroderma much earlier.
Diagnosing Scleroderma
A rheumatologist or a dermatologist can diagnose and treat scleroderma.
Properly diagnosing scleroderma involves the following:
- Healthcare Assessment: A healthcare practitioner will evaluate current symptoms and health history with an individual who is suspected of having scleroderma. The healthcare practitioner will also ask about a family history of any autoimmune or related diseases.
- Physical Examination: A healthcare practitioner will take a look from head to toe for any physical symptoms that may be present.
- Skin Biopsy: Examining an area of affected skin under a microscope will help the healthcare practitioner with a diagnosis. The practitioner will quickly remove a very small area of the skin for examination.
- Blood Tests: A blood test can check for elevated levels of antinuclear antibodies (ANA), which are often present in 80% of those with scleroderma (95%+ for those with lupus). In a 2015 Seminars in Arthritis and Rheumatism article, researchers found that individuals who were ANA negative experienced fewer occurrence of pulmonary arterial hypertension, spider veins (telangiectasias), gastrointestinal issues and skin ulcers. Testing for anti-centromere antibodies (ACA) and anti-Scl-70 antibodies is also very useful in distinguishing patients with systemic sclerosis (SSc) from patients with other connective tissue diseases.
- Other Lab Tests: Lab tests may be ordered and conducted to evaluate systemic and organ involvement and include X-rays, MRIs and/or CAT scans to determine the extent of the disease.
In 2013, the American College of Rheumatology in partnership with the European League Against Rheumatism agreed on a set of criteria to help practitioners diagnose SSc. Each symptom is weighted and if the score is at least 9 or greater, the individual most likely has SSc. If an individual has thickening of the fingers on both hands and the thickening extends to the metacarpophalangeal joints (the joints at the bottom of fingers where they meet the palm), then that criteria alone is enough to diagnose SSc.
The criteria is as follows:
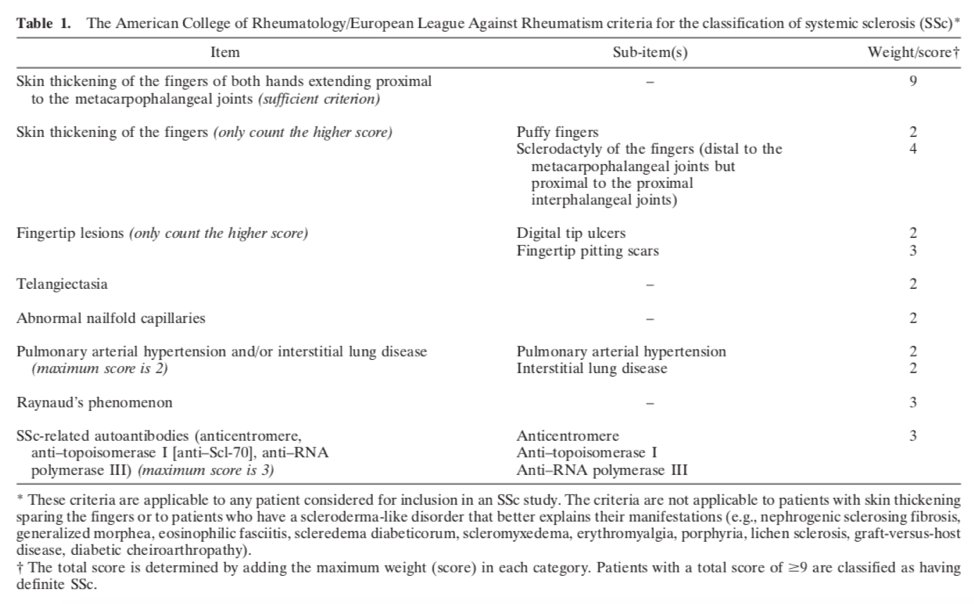

Image sourced from Medical News Today
Treating Scleroderma
Some treatments for scleroderma, especially those related to symptoms of inflammation, are quite similar to those for lupus – though there are also several differences. According to the American Academy of Dermatology (AAD) and Harvard Health, the following are effective drug treatments for scleroderma and its symptoms:
- Methotrexate: An anti-rheumatic, methotrexate can help reduce pain and swelling due to inflammation. Results of a small 2012 study show that individuals with localized scleroderma who were prescribed methotrexate along with a corticosteroid (prednisone) for 36 months did not experience a scleroderma flare during that time showing methotrexate is typically well-tolerated and effective.
- Immunosuppressive therapy: Immunosuppressives, such as mycophenolate mofetil (CellCept), mycophenolate sodium (Myfortic), cyclosporine and cyclophosphamide (Cytoxan) can help regulate the immune system and even help improve lung function in individuals who experience lung and pulmonary involvement.
- Angiotensin converting enzyme (ACE) inhibitors: ACE inhibitors, such as enalapril and lisinopril, can help lower blood pressure and possibly help protect the kidneys from damage.
- Vasodilators: Vasodilators, such as treprostinil and inoprost, may treat pulmonary hypertension, and the symptoms of Raynaud’s phenomenon as well.
- Calcipotriene: A synthetic form of vitamin D, calcipotriene is used topically to treat skin and regulate the growth and production of skin cells.
- Corticosteroids: Medications, such a prednisone, can help reduce inflammation.
- Imiquimod: A common treatment for some skin cancers and genital warts, imiquimod is applied topically and induces interferon to treat skin manifestations (morphea).
- Tacrolimus ointment: A topical treatment, tacrolimus can be prescribed for inflammation, redness and itching of the skin when other treatments fail to work.
- Non-steroidal anti-inflammatory drugs (NSAIDs): NSAIDs such as ibuprofen may help with joint inflammation and discomfort.
- Diuretics: Used to release excess fluid, diuretics may be effective in relieving swollen hands and feet and bring relief.
- Acid reducers (e.g. omeprazole): Acid reducers may help alleviate heartburn and treat esophageal symptoms.
Other treatments may include:
- Phototherapy: UVA-1 phototherapy may be prescribed to treat morphea that is deep. Narrow-band UVB therapy may help with morphea that only affects the top layers of skin. Intense pulsed light treatments (IPL) may help reduce skin discoloration and hyperpigmentation.
- Physical therapy: A physical therapist can help an individual with scleroderma maintain and increase mobility where skin has thickened.
- Moisturizers: Regular application of moisturizers can help control itch and help heal dry skin.
- Warm water soaks: Soaking in warm water can help reduce calcium deposits under the skin that may develop with scleroderma.
In Conclusion
As with lupus, scleroderma is a serious, life-altering autoimmune condition with currently no cure. As overlap diseases, they share some symptoms that can make differential diagnosis tricky. However, this also means that there are treatment options that can reduce these same symptoms in those who are diagnosed with both. If you have scleroderma, work closely with your healthcare practitioner, and advocate for yourself to ensure that you receive the best care possible. That will go a long way in minimizing or even preventing organ damage and increasing your quality of life!
References
Alharbi, S., Ahmad, Z., Bookman, A., Touma, Z., Sanchez-Guerrero, J., Miksakakis, N., & Johnson, S. (2018). Epidemiology and survival of systemic sclerosis-systemic lupus erythematosus overlap syndrome. The Journal of Rheumatology, 45(10), 1406-1410. doi: 10.3899/jrheum.170953.
Higgs, B, Liu, Z., White, B., Zhu, W., White, W., Morehouse, C., Brohawn, P., Kiener, P., Richman, L, Fiorentino, D., Greenberg, S., Jallal, B., & Yao, Y. (2011). Patients with systemic lupus erythematosus, myositis, rheumatoid arthritis and scleroderma share activation of a common type 1 interferon pathway. Annals of the Rheumatic Diseases, 2011(70), 2029-2036. doi: 10.1136/ard.2011/150326. Retrieved March 26, 2020 from https://www.researchgate.net/profile/Peter_Kiener2/publication/51535029_Patients_with_systemic_lupus_erythematosus_myositis_rheumatoid_arthritis_and_scleroderma_share_activation_of_a_common_type_I_interferon_pathway/links/53fe640e0cf23bb019be4a70/Patients-with-systemic-lupus-erythematosus-myositis-rheumatoid-arthritis-and-scleroderma-share-activation-of-a-common-type-I-interferon-pathway.pdf
Jaeger, V., Wirz, E., Allanore, Y., Rossbach, P., Riemekasten, G., Hachulla, E., Distler, O., Airò, P., Carreira, P., Balbir Gurman, A., Tikly, M., Vettori, S., Damjanov, N., Müller-Ladner, U., Distler, J., Li, M., Walker, U., & EUSTAR co-authors. (2016). Incidences and risk factors o organ manifestations in the early course of systemic sclerosis: A longitudinal EUSTAR study. PLoS ONE 11(10), e0163894. doi: 10.1371/journal.pone.0163894.
Limited scleroderma. (n.d.). Mayo Clinic. Retrieved March 26, 2020 from https://www.mayoclinic.org/diseases-conditions/crest-syndrome/symptoms-causes/syc-20355535
Niklas, D., Niklas, A., Majewski, D., & Puszczewicz. (2016). Rheumatic diseases induced by drugs and environmental factors: The state-of-the-art – part one. Reumatologica, 54(3), 122-127. doi: 10.5114/reum.2016.61212. Retrieved March 26, 2020 from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4967979/pdf/RU-54-27993.pdf
Pediatric systemic scleroderma. (2020). Cleveland Clinic. Retrieved March 26, 2020 from https://my.clevelandclinic.org/health/diseases/4910-pediatric-systemic-scleroderma
Renal involvement in scleroderma. (2020). University of Michigan. Retrieved March 26, 2020 from https://www.uofmhealth.org/conditions-treatments/rheumatology/renal-involvement-scleroderma
Salazar, G., Assassi, S., Wigley, F., Hummers, L., Vargas, J., Hinchcliff, M., Khanna, D., Schiopu, E., Phillips, K., Furst, D., Steen, V., Baron, M., Hudson, M., Taillefer, S., Pope, J., Jones, N., Docherty, P., Khalidi, N., Robinson, D., Simms, R., R, Silver. …Mays, N. (2015). Antinuclear antibody negative systemic sclerosis. Seminars in Arthritis & Rheumatism, 44(6), 680-686. doi: 10.1016/j. semarthrit.2014.11.006. Retrieved March 26, 2020 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4447614/pdf/nihms645897.pdf
Scleroderma. (n.d.). Mayo Clinic. Retrieved March 26, 2020 from https://www.mayoclinic.org/diseases-conditions/scleroderma/symptoms-causes/syc-20351952
Scleroderma. (2018). Harvard Health Publishing. Retrieved March 26, 2020 from https://www.health.harvard.edu/a_to_z/scleroderma-a-to-z
Scleroderma: Diagnosis and treatment. (2020). American Academy of Dermatology Association. Retrieved March 26, 2020 from https://www.aad.org/public/diseases/a-z/scleroderma-treatment
Scleroderma in children. (2020). Stanford Children’s Health. Retrieved March 26, 2020 from https://www.stanfordchildrens.org/en/topic/default?id=scleroderma-in-children-90-P01729
Scleroderma risk factors. (2020). Johns Hopkins Medicine. Retrieved March 26, 2020 from https://www.hopkinsmedicine.org/health/conditions-and-diseases/scleroderma/scleroderma-risk-factors
Skin lupus and scleroderma. (2020). Yale Medicine. Retrieved March 26, 2020 from http://www.jrheum.org/content/jrheum/45/10/1406.full.pdf
Systemic scleroderma. (n.d.). U.S. National Library of Medicine. Retrieved March 26, 2020 from https://ghr.nlm.nih.gov/condition/systemic-scleroderma#genes
Torok, K., & Arkachairsri, T. (2012). Methotrexate and corticosteroids in the treatment of localized scleroderma: A standardized prospective longitudinal single-center study. Journal of Rheumatology, 39(2), 286-294. Doi: 10.3899/jrheun.110210. Retrieved March 26, 2020 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3744892/
Types of scleroderma. (2020). Johns Hopkins Medicine. Retrieved March 26, 2020 from https://www.hopkinsmedicine.org/health/conditions-and-diseases/scleroderma/types-of-scleroderma
Understanding scleroderma. (2020). Johns Hopkins Scleroderma Center. Retrieved March 26, 2020 from https://www.hopkinsscleroderma.org/scleroderma/
van den Hoogen, F., Khanna, D., Fransen, J., Johnson, S., Baron, M., Tyndall, A., Matucci-Cerinic, M., Naden, R., Medsger Jr., T., Carreira, P., Riemekasten, G., Clements, P., Denton, C., Distler, O., Allanore, Y., Furst, D., Gabrielli, A., Mayes, M., van Laar, J., Seibold, J., Czirjak, L., …Pope, J. (2013). 2013 classification criteria for systemic sclerosis. Arthritis & Rheumatism, 65(11), 2737-2747. doi: 10.1002/art.28098. Retrieved March 26, 2020 from https://onlinelibrary.wiley.com/doi/pdf/10.1002/art.38098
What is scleroderma? (2020). Scleroderma Foundation. Retrieved March 26, 2020 from https://www.scleroderma.org/site/SPageNavigator/patients_whatis.html#.XnvI8xNKh0t
Author: Liz Heintz
Liz Heintz is a technical and creative writer who received her BA in Communications, Advocacy, and Relational Communications from Marylhurst University in Lake Oswego, Oregon. She most recently worked for several years in the healthcare industry. A native of San Francisco, California, Liz now calls the beautiful Pacific Northwest home.
All images unless otherwise noted are property of and were created by Kaleidoscope Fighting Lupus. To use one of these images, please contact us at [email protected] for written permission; image credit and link-back must be given to Kaleidoscope Fighting Lupus.
All resources provided by us are for informational purposes only and should be used as a guide or for supplemental information, not to replace the advice of a medical professional. The personal views expressed here do not necessarily encompass the views of the organization, but the information has been vetted as a relevant resource. We encourage you to be your strongest advocate and always contact your healthcare practitioner with any specific questions or concerns.