
Lupus Nephritis
Lupus nephritis (LN) is a leading cause of death in SLE and can affect from 40% to 50% of those with lupus. Yet, newly approved drug therapies promise to change the future LN. Read on to learn more about this dangerous condition and how it can be treated.
- Introduction: What is lupus nephritis?
- Who is at the greatest risk for developing lupus nephritis?
- How is lupus nephritis diagnosed and treated?
- What can I do to keep my kidneys healthy?
- In Conclusion
.

Introduction: What is lupus nephritis?
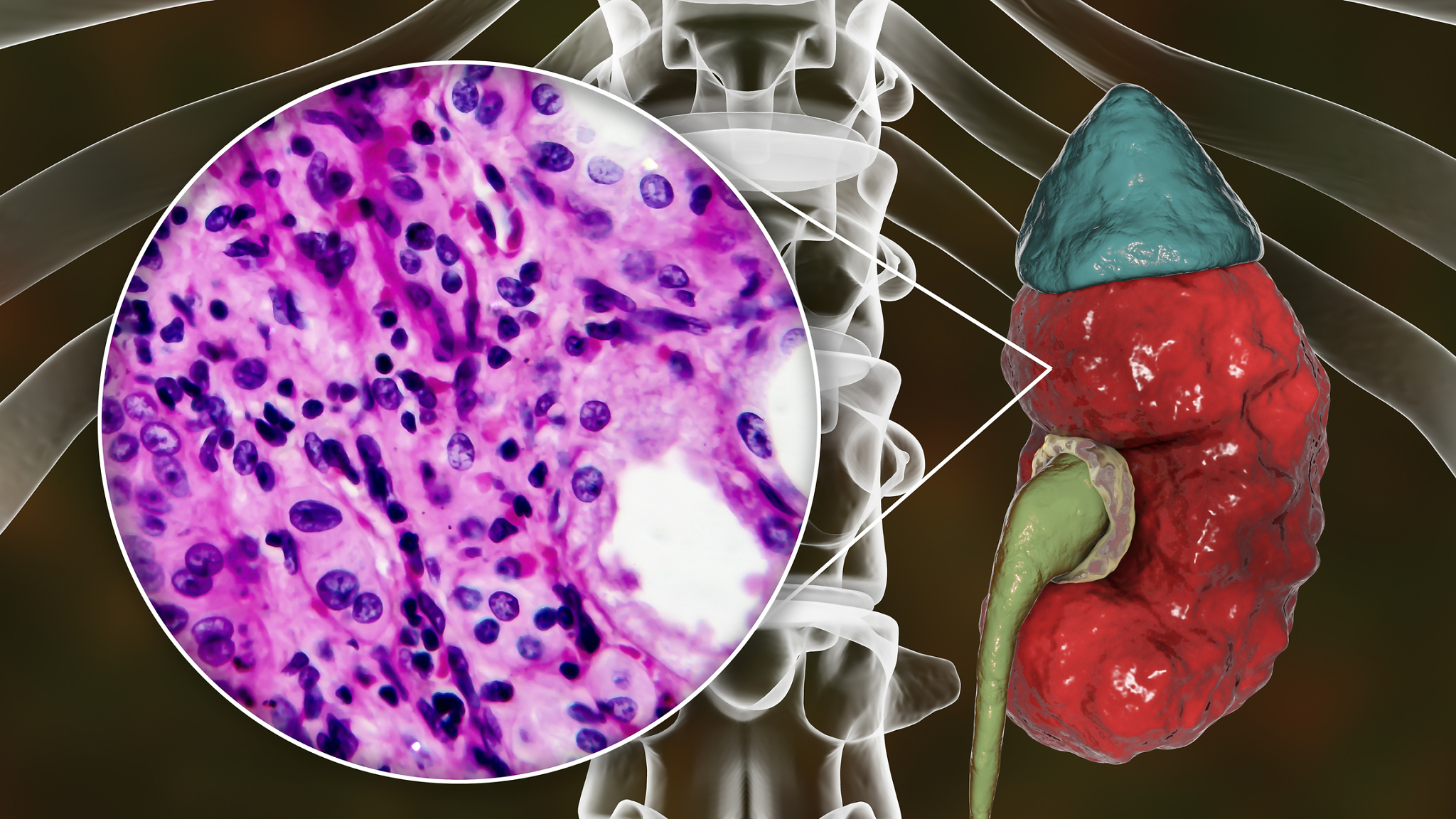
LN is an inflammatory condition caused by SLE. There are small blood vessels in the kidneys called glomeruli (plural for glomerulus) that does the important work of filtering waste and fluid from the blood in the kidneys. Antibodies may start attacking these glomeruli, causing inflammation, swelling, and scarring, which in turn may cause small blood clots to form. It’s the formation of these blood clots that eventually trigger the following LN symptoms:
- swelling in the extremities and weight gain;
- blood and/or protein in the urine; and
- high blood pressure.
If these symptoms are ignored and not quickly and adequately treated, LN can potentially be life-threatening.
It is unclear what causes LN, though genetics, infections, viruses, and the environment may play roles. Recent studies suggest that gut health and the microbiome may even play a role in LN development, as an imbalance of intestinal bacteria has also been linked to increased lupus disease activity. Cellular inflammation of the kidney
Like lupus, there is no cure for LN (yet!). For now, the goals of treating LN include reducing symptoms – hopefully within 12 months – and achieving and maintaining remission. LN can often be managed through good nutrition and medication, though it may require dialysis. A kidney transplant may be necessary if the condition causes kidney failure. However, there is good news – the five-year survival rate for LN has increased over the years to a little less than 90% and a complete remission rate of just under 60%.
While it may be hard to determine whether or not you will get LN, you can work closely with a healthcare practitioner to stay on top of kidney health. You can also do things – like breaking old habits or developing new ones – that can help you and your kidneys stay as healthy as possible when you have lupus.
Who is at the greatest risk for developing lupus nephritis?
Anyone who has SLE may possibly get LN, and the risk increases with age. However, the following groups have been identified as being at exceptionally high risk:
- men, who experience worse symptoms than women;
- African Americans and Asian/Pacific Islanders, who are at four times greater risk;
- Hispanics and Native Americans, who are at two times greater risk; and
- Young people with lupus under the age of 30 and children – LN may even be the initial symptom of SLE for them.
It is not completely clear what role ethnicity plays in the development of LN. Lower socioeconomic status, which is often linked with ethnicity, may influence who gets LN and to what degree, and there may be some genetic factors. It’s cause for concern and deserves more aggressive research and study. This information can shape how LN and lupus are treated in the future, especially those who are exceptionally vulnerable and who may not typically receive adequate care.
It’s always best to talk to your healthcare practitioner about your unique concerns and risks so you both can take a more proactive approach towards your healthcare. LN can also put you at risk for developing heart problems, blood vessel problems, and even B-cell lymphoma, making it imperative to stay on top of kidney health.

How is lupus nephritis diagnosed and treated?
Diagnosis
A nephrologist will use the following diagnostic tools to check the health of your kidneys:
- a urinalysis to check for protein and blood in the urine, which are often the first indications of damage;
- blood tests to see how well your kidneys are filtering fluids and removing wastes;
- tests to check for antiphospholipid antibodies and anti-nuclear antibodies; and possibly
- a kidney biopsy to look for direct signs of kidney damage.
The severity of LN is determined by using the following class system:
Class 1: Minimal Mesangial Glomerulonephritis: Minimal kidney damage with minimal symptoms.
Class 2: Mesangial Proliferative Glomerulonephritis: An area of the kidney may show LN, and there may be blood and protein in the urine.
Class 3: Focal Glomerulonephritis: There is less than 50% damage to the main blood vessels of the kidney. There may be blood/protein in the urine, and blood pressure may be high.
Class 4: Diffuse Proliferative Glomerulonephritis: There is more than 50% damage to the kidney’s main blood vessels, and there may be kidney damage. Kidney function may also be impaired, and blood pressure may be high.
Class 5: Membranous Glomerulonephritis: Symptoms from classes 3 and 4 may be present and hardening of the vessels in the kidneys, and it may be time for dialysis or even a transplant.
Class 6: Advanced Sclerotic: More than 90% of the kidney’s major vessels are damaged, and it may be time for dialysis or a transplant.
Treatment
Lupus nephritis is treated according to the severity of symptoms. In very mild cases, you may just have to make some dietary changes. Drug treatment is the next step. These may be similar to medications that may already be used for lupus or other unrelated kidney conditions: These standard therapies include:
- corticosteroids (prednisone and methylprednisolone);
- immunosuppressives (cyclophosphamide, azathioprine, mycophenolate mofetil, and hydroxychloroquine);.
- blood pressure medications; and
- diuretics to release excess fluids.
Most recently, however, and for the first time, two immunosuppressant medications have been specifically approved by the US Food and Drug Administration (FDA) for treating LN in adults in the U.S.!
Benlysta (belimumab) was the first drug ever designed and approved for SLE (2011). It is a biologic (a monoclonal antibody) that was the first drug specifically designed and approved to treat SLE. It is given intravenously, and since 2019, has been approved for children 5 years of age or older. It is given with other standard therapies. In 2020, after two years of clinical trials, Benlysta significantly reduced kidney disease activity and was given FDA approval.
LUPKYNIS (voclosporin) is a novel medication developed from the start to specifically treat LN. Lupkynis works by blocking a protein in the immune system called calcineurin, which in turn stops T cells from triggering an autoimmune response. In some studies, 40.8% of participants given voclosporin achieved complete kidney response. Lupkynis is given as an oral dose and should not be prescribed with cyclophosphamide. Lupkynis was approved for the treatment of lupus nephritis in 2021.
Between 10-30% of those with LN don’t respond to treatment and eventually need dialysis to properly filter fluids and blood. Others may need a kidney transplant. Hopefully, the addition of belimumab and voclosporin will help increase the odds against these more invasive measures!
What can I do to keep my kidneys healthy?
While you can’t necessarily prevent LN, there are things you can do while working with your practitioner to make sure you are doing all you can to keep your kidneys healthy. This includes:
Making Dietary Changes: A nutritionist can help you choose foods that are low in salt and sodium and are not processed. Eating lean proteins, smaller portions of protein-rich foods, fruits and vegetables, and low-fat dairy is also recommended.
Exercising: Exercising to your ability can help reduce stress, promote heart health, promote better sleep, and control weight. Find the exercise routine that works best for you – it doesn’t have to be complicated or aggressive.
Taking Care of Emotional Well-being: Relieve stress with things such as mindfulness meditations, acupuncture, or mental health therapy. There are lots of things that you may already do that are great for relieving stress.
Improving Sleep: Sleep plays a huge role in how we feel. Make sure that you are getting healthy sleep by limiting caffeine, alcohol, and nicotine. Avoid blue light devices right before bed, and create a cozy and comfortable sleep environment that promotes rest.

Developing greater awareness about kidney health can help you talk with your healthcare practitioner about any concerns and risks you may have. While LN may not be predictable or preventable, you can do all you can to stay as healthy as possible to increase your odds against developing severe outcomes and complications from kidney disease.
References
Azzouz, D., Omarbekova, A., Heguy, A., Schwudke, D., Gisch, N., Rovin, B., Caricchio, R., Buyon, J., Alekseyenko, A., & Silverman, G. (2019). Lupus nephritis is linked to disease-activity associated with expansions and immunity to a gut commensal. Annals of Rheumatic Diseases,78, 947-956. https://doi.10.1136/annrheymdis-2018-214856
Gasparotto, M., Gatto, M., Binda, V., Doria, A., and Moroni, G. (2020). Lupus nephritis: Clinical presentations and outcomes in the 21st century. Rheumatology, 59(5), 39-51. https://doi.org/10.1093/rheymoatology/keaa381
Inacio, P. (27, March 2020). Voclosporin helps protect kidneys in lupus nephritis, pase 3 trial shows. Lupus News Today. https://lupusnewstoday.com/2020/03/27/voclosporin-plus-standard-care-therapy-doubles-kidney-responses-lupus-nephritis-aurora-trial/#:~:text=In%20total%2C%2040.8%25%20of%20patients,likelihood%20of%20a%20complete%20response.
LUPKYNIS is the first FDA-approved oral treatment specifically for lupus nephritis. (2021). Lupkynis. https://www.lupkynis.com/?fbclid=IwAR2FhWLHzzd_C-VrxNBdimzIMxE63ODcBzTMTnIg1iwXhoHdban6AKE2w5Q
Lupus and kidney disease (lupus nephritis). (2017). National Institute of Diabetes and Digestive and Kidney Diseases. https://www.niddk.nih.gov/health-information/kidney-disease/lupus-nephritis#what
Samotij, D. & Reich, A. (2019). Biologics in the treatment of lupus erythematosus: a critical literature review. BioMed Research International. https://doi.org/10.1155/2019/8142368
Understanding lupus nephritis. (2021). All In. https://www.allinforlupusnephritis.com/about-lupus-nephritis
Author: Liz Heintz and the KFL Team
Liz Heintz is a technical and creative writer who received her BA in Communications, Advocacy, and Relational Communications from Marylhurst University in Lake Oswego, Oregon. She most recently worked for several years in the healthcare industry. A native of San Francisco, California, Liz now calls the beautiful Pacific Northwest home.
All images, unless otherwise noted, are property of and were created by Kaleidoscope Fighting Lupus. To use one of these images, please contact us at [email protected] for written permission; image credit and link-back must be given to Kaleidoscope Fighting Lupus.
All resources provided by us are for informational purposes only and should be used as a guide or for supplemental information, not to replace the advice of a medical professional. The personal views expressed here do not necessarily encompass the views of the organization, but the information has been vetted as a relevant resource. We encourage you to be your strongest advocate and always contact your healthcare practitioner with any specific questions or concerns.